
The Devilish Details of Data Collection
A Primer On How Quality Reporting Works In HealthCare

In my last article and video, I discussed the quality of quality measures, i.e., how quality metrics generally don't measure the quality of care they were designed to measure. In our quest for better quality, PCPs face a growing administrative burden: collecting and reporting data to prove they provide good quality care. This article explores what the quest for quality looks like for PCPs—from navigating complex coding systems to adopting emerging data standards.
The video version of this article is embedded below and on my YouTube Channel.
Audio podcast and Video versions are also available on the Podcasts Page.
NCQA
The National Committee for Quality Assurance (NCQA) is a non-profit organization established in 1990 to measure, analyze, and report how well health organizations provide “scientifically recommended care.”
To achieve this objective, NCQA sets the standards for quality measures in healthcare. These standard metrics are called Healthcare Effectiveness Data and Information Set (HEDIS). NCQA certifies healthcare entities (for a fee) that they are following the HEDIS methodology to collect data and use standardized logic to calculate and report metrics. This certification ensures that quality performance can be compared across health organizations.
While CMS still defines some metrics, it borrows heavily from NCQA, and most metrics used in CMS quality reporting programs follow the HEDIS methodology.
Anatomy of a Quality Metric
The anatomy of a typical quality metric includes the following:
Measure: The “appropriate process” or outcome that is being measured.
Denominator: This defines the total number of patients eligible for the specified measure, i.e., the population to which the metric applies.
E.g., Everyone between the age of 18-75 and a prior diagnosis of diabetes.
Numerator: Total number of people that meet the specific criteria defined by the measure that will enable the patient (and doctor) to meet the quality metric.
E.g., Everyone in the denominator that has a HbA1c < 9%
Exclusion: These define the specific reasons why a patient who was part of the initial population (denominator), should not be included in the final calculation of the metric, i.e., conditions that would “disqualify” the patient from being counted.
E.g., A person who is enrolled in hospice
Reporting Period: The timeframe over which data is collected and the metric is calculated.
E.g., Jan 1 to Dec 31 for diabetes control, i.e., HbA1c < 9%
Data Source: The source from which the data used to calculate the metric is obtained. Examples include:
Lab value for HbA1c
Billing codes for Diabetes eye exams or colonoscopy
Diabetes eye exam or colonoscopy report
Even with this basic understanding of the anatomy of quality metrics, you can imagine why collecting accurate quality data is challenging and time-intensive.
Insurance companies often inform PCPs of the “gaps in care” by sending faxed patient lists or using MS Excel spreadsheets. Since insurance companies often lack all this data, their reported quality data often fails to reflect true quality levels.
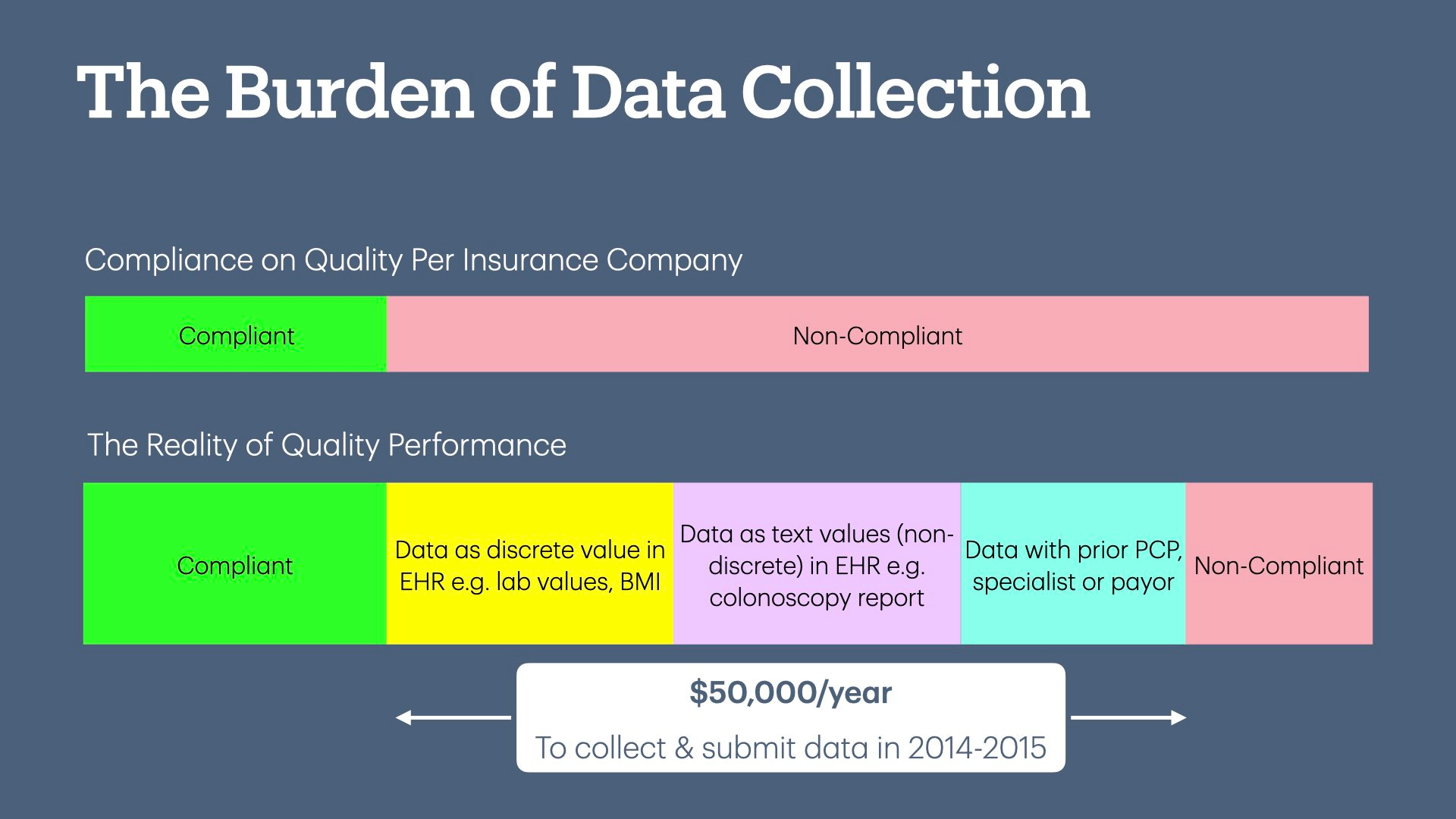
To collect and report this data back to insurance companies, PCP offices spent approximately $50,000 in 2014-2015.1 This is why larger organizations with an army of data analysts will always perform better than small medical practices—they have the money and resources to collect and report data.
I concluded in my last article, “The Quality of Quality Measurement:”
The question then is, why are we subjecting healthcare providers to this data collection exercise? The answer lies in Value-Based Contracts—these metrics have become a mechanism for increasing health insurance company profits.
Now that we understand how quality metrics are structured, below we will delve into the devilish details of data sources and collection methods that PCPs must use to prove that they are rendering good-quality care.
(Coming up: CPT & ICD-10 codes, CPT-II codes, supplemental data, and emerging standards such as eCQM, QRDA, and dQM)
CPT and ICD-10 Codes
CPT (Current Procedural Terminology) Codes are a set of medical codes used to describe medical, surgical, and diagnostic services provided to patients for billing purposes.
99214 (Office or other outpatient visit for the evaluation and management of an existing patient). This CPT code requires a doctor to take/perform a medically appropriate history and/or examination, and the case complexity is at a moderate level of medical decision-making.
ICD-10 (International Classification of Diseases, 10th Revision) is a set of diagnosis codes that represent medical diseases or symptoms. Medical providers use these codes when billing for services to tell the insurance company the reason for performing the service.
E11.9 - Type 2 Diabetes Mellitus without complications
Therefore, if an established patient were seen by their doctor for an office visit, you would see the two codes on your EOB (Explanation of Benefits):
99214, i.e., the office visit service.
E11.9, i.e., the office visit was to evaluate diabetes.
Let us take the example of diabetes eye exam screening to screen for retinopathy. To define the population, i.e., denominator, a person needs to be evaluated and treated for diabetes within a timeframe. Therefore, we need:
All CPT codes that are used for medical evaluation by a provider (e.g., office visits)
One way to satisfy the diabetic eye exam measure (be counted in the numerator) is through an ophthalmologist visit specifically for diabetes. The ophthalmologist would then bill the insurance company using codes like CPT 92014 (office visit for eye exam) and ICD-10 E11.9, indicating the measure has been met.
However, if the patient switches insurance plans (or has a vision-only plan), the new insurance company may not have the CPT and ICD-10 codes from the ophthalmologist. The PCP now has the burden of proving that the patient had a diabetic eye exam, i.e., the PCP office has to collect “supplemental data” and submit it to the insurance company.
Furthermore, when the numerator requires lab values or other discrete data from the medical chart (e.g., BMI, BP values), traditional CPT and ICD-10 codes may not be sufficient.
CPT-II Codes
CPT-II codes are $0 supplemental quality codes submitted to insurance companies as part of the office visit bills. These codes indicate to the insurance that the patient should be counted in the numerator.
For example, here are the codes for diabetes HbA1c control:
3044F: The most recent HbA1c level is less than 7.0%
3051F: The most recent HbA1c level is greater than or equal to 7.0% and less than 8.0%
3052F: The most recent HbA1c level is greater than or equal to 8.0% and less than or equal to 9.0%
3046F: The most recent HbA1c level is greater than 9.0%
The AMA developed these codes to decrease the need for medical record abstraction and chart review, which would hopefully decrease the administrative burden on physicians. However, using and submitting these codes comes with its own set of challenges.
CMS has HCPCS Level II codes, similar to CPT-II codes, that serve the same purpose.
Submitting both CPT-I and CPT-II after an Office Visit
Due to the diverse conditions we treat, PCPs use a wide range of CPT and ICD-10 codes. The rules and regulations of these codes change frequently, and the rules may be different for different insurance companies. CPT-II codes follow the same patterns. Using CPT-II codes takes additional time if PCPs enter these codes in the EHR themselves or if they need to hire a credentialed biller. This increases overhead costs. Furthermore, even though the codes themselves are standardized, each insurance plan makes its own decision on which codes it will accept. In practice, PCPs submit CPT-II codes without knowing which, if any, insurance plan will give them credit.
Some EHRs have tried to automate billing CPT-II codes to make the workflow easier for PCP offices.2 This works well for discrete values in the EHR, e.g., HbA1c documented in the lab value field, but falls apart if the HbA1c value is in the endocrinologist’s note that was faxed to PCP—remember, PCP is responsible for submitting this data.
But Wait—We Can't Submit More Codes.
The CMS-1500 form, which is used to submit bills, has space for only six CPT codes.

Since sick patients may undergo multiple office-based tests, all six lines can be used by CPT-I codes to bill for the service that was rendered. This leaves no space for transmitting CPT-II codes to the insurance company. The ANSI X12 electronic billing standard attempts to solve this problem as, technically, there is no limit to the number of CPT codes the EHR can submit—however, then you run into issues with the clearing house3 and health insurance plans ability to process codes. If the provider submits more than six CPT codes, there is no guarantee that these codes will reach the insurance company or will be processed to give credit for meeting the quality metric.
Impact on Quality due to Claim Rejections
Payors routinely deny claims for “Unspecified and complex” reasons. All CPT codes, including CPT-II codes, are generally denied when a claim is denied. These claim denials prevent the PCP office from reporting that they met the quality metric.
Supplementary Data
Some health plans (depending on negotiation) may accept supplemental data to allow the PCP office to prove that they met the metrics. Every insurance plan defines the quality metric for which it will accept supplemental data and the format in which it will accept it.
Spreadsheet—CSV or Excel Files
The insurance company defines the formatting of the CSV or Excel files that a PCP office can use to submit supplemental data (i.e., data elements, headers, columns, data format, etc). This allows the insurance company to ingest the supplemental data into their database to credit the PCP. However, each insurance company requests CSV files in a different format, even for the same metric. For example, Aetna and United may want a different CSV format for HbA1c values. EHRs are not designed for this function, so the PCP office must now build or buy a data warehouse technology to submit this data to different insurance companies.
Here is an example of an Excel request from the State of CT that I received during the height of the COVID-19 pandemic. This is to give you an example of the type of requests we get.4
Chart Abstraction
Since patients often change insurance plans, the new plans will request copies of the medical records as proof that the person underwent the care to close the gap in the quality metric, such as colonoscopy and mammogram reports.
In real life, this increases the workload on the PCP office dramatically, as they are responsible for closing the “gaps in care.” A PCP office will routinely receive a list of patients from various insurance companies to submit records, especially for Medicare Advantage plans, where the insurance company needs to meet its Star ratings to get money from CMS. This workflow typically involves:
Find the requested documentation in the patient's chart (e.g., colonoscopy or mammogram report).
Call other medical offices (e.g., specialists, prior PCP, radiology centers) to collect the medical records.
Collate these records by the insurance company and either fax or upload them to a designated website.
While carrying out the above workflow, the office also needs to ensure that the request is legitimate to comply with HIPAA—and yes, offices receive requests for medical records from fraudulent companies. This verification of medical record requests is often complicated because insurance companies often don’t request the medical records directly but contract it out to third-party companies. Often, there is no good way to verify if the request is legitimate without spending an inordinate amount of time—calling the insurance company and waiting 30-60 min on hold to reach the “first level support” is useless as they have no idea.
The industry has no idea how many medical record requests are released to fraudulent companies posing as health plan agents. Small practices are aggressively penalized for not submitting records, so they err on the side of releasing them.
Emerging/New Standards: eCQM, QRDA, and dQM
Given the exorbitant cost of reporting quality measures for physician practices,5 there is a movement to “computerize” the collection and calculation of quality measures, which hopes to reduce the burden of quality measurement. While this topic is a whole newsletter in itself, below is a summary.
Electronic Clinical Quality Measures (eCQM)6
eCQMs attempt to measure quality by computerizing the logic of all the elements I discussed in the anatomy of quality metrics above—denominator, numerator, exclusions, reporting period, and data source.
The central problem with eCQM is that while the logic may be accurate, it is only as good as the data fed into it. Therefore, it does not solve the data abstraction problem; it just changes how you report it.
For example, eCQM can develop the logic to meet the criteria for colon cancer screening, but if the data does not exist in the PCP's EHR, the PCP office still needs to source the colonoscopy report. eCQM changes how a PCP office will submit this report: instead of faxing (or uploading) the report to the insurance company, the PCP office may have to follow the EHR best practice to trigger the eCQM logic.
Quality Reporting Document Architecture (QRDA)7
If you are familiar with the Clinical Document Architecture (CDA) standard8 for exchanging clinical data using Health Information Exchange (HIE)—QRDA is the CDA equivalent for exchanging quality data.
According to the HealthIT.gov website:
QRDA I is an individual patient-level report used by eligible hospitals (EHs) to submit data to CMS.
QRDA III is an aggregate quality report used by eligible clinicians to submit data to CMS for the entire medical practice.
Essentially, QRDA uses a standardized format to transmit quality data from the EHR to the payor.
Since PCPs bear the burden of reporting quality metrics, PCP offices (or ACOs) will have to use QRDA III to submit data to CMS, in addition to the other methods described above, as not all quality measures are in eCQM format. As it stands, eCQM and QRDA III data submission creates an uneven playing field and penalizes independent PCPs. Large organizations that use the same EHR across all specialties will have more data in the same system, making it easier for them to submit data. Since payments are increasingly tied to quality, small independent practices will end up with reduced reimbursements due to reporting challenges.
Digital Quality Measures (dQM)9
dQM takes eCQM one step further by using data from disparate health systems, not just the EHR, to measure quality. These other systems may include health information exchange (HIE), payor claims data, care coordination systems, state immunization registries, etc. The biggest benefit of dQM is that it reduces the burden on primary care by using standard data-sharing protocols (such as FHIR) to collect data from other health systems that may not exist in PCPs’ EHR.
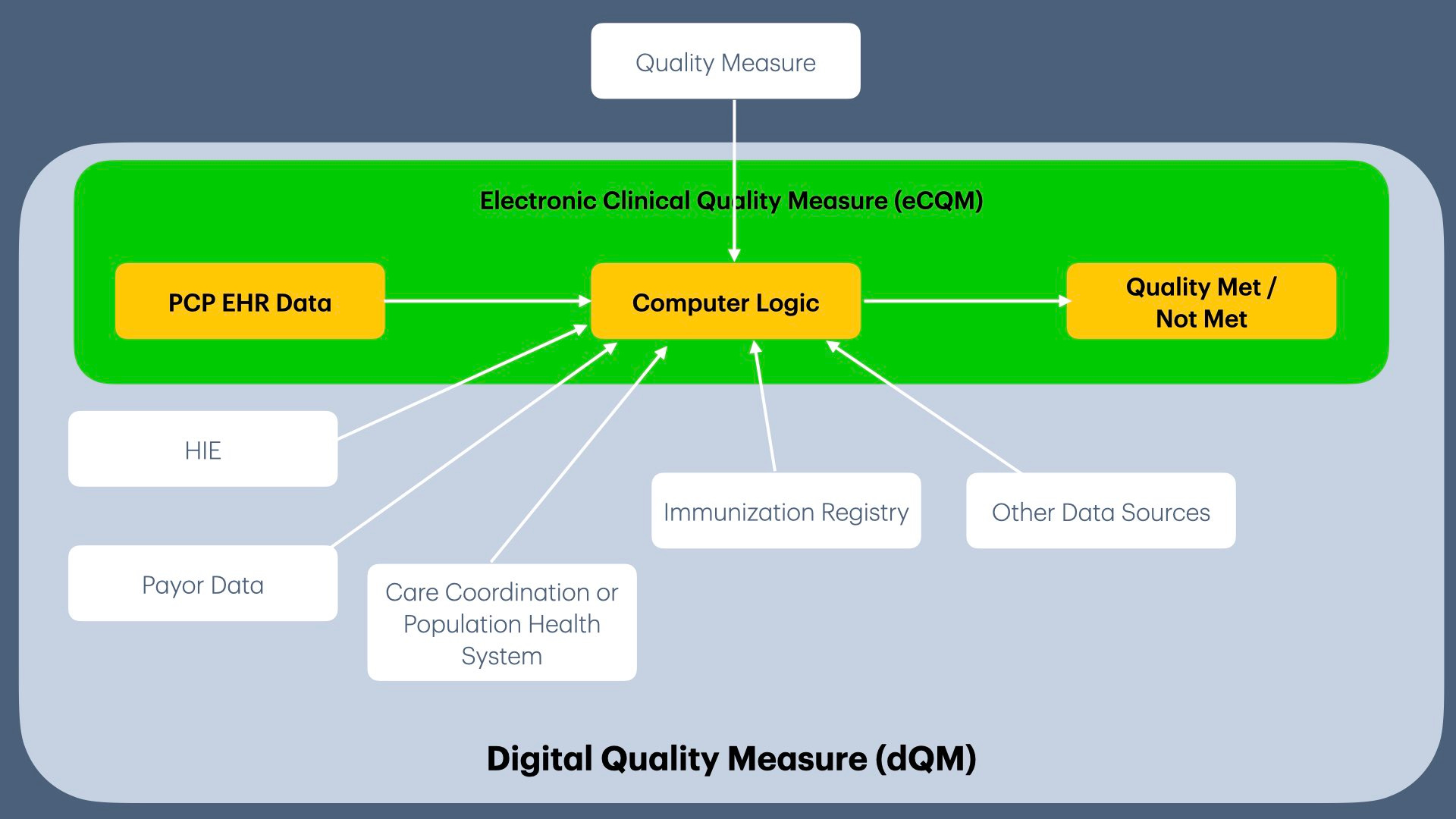
For example, if a PCP does not have a colonoscopy report in their EHR, dQM could automatically retrieve it from the HIE and credit the PCP.
Electronic Clinical Data System (ECDS)
Per NCQA, an “Electronic Clinical Data System” will collect, compute, and submit data to NCQA. It is an open question whether “this system” will be EHRs or whether organizations will need to maintain a separate system for quality reporting.
eCQM and dQM appear to improve on the current data collection methods, but it has taken us over 10 years to implement CDA (remember, QRDA is similar to CDA). CDA is still bogged down by standardization (even though it is a standard), as different health systems have their own version of CDA. We risk going down the same path with QRDA. Furthermore, small practices are already spending a small fortune on EHRs. Adding the requirement of purchasing and maintaining ECDS may push them to the brink of bankruptcy. We are starting the long and arduous journey of eCQM and dQM for data collection and reporting while AI lurks around the corner.
Up Next
Now that we understand the anatomy of a quality metric and how data is collected, we will examine the “BMI Screening and Follow-Up Plan” metric in detail in the next article & video.
If you liked this article, please consider sharing it.
Casalino, L. P., Gans, D., Weber, R., Cea, M., Tuchovsky, A., Bishop, T. F., Miranda, Y., Frankel, B. A., Ziehler, K. B., Wong, M. M., & Evenson, T. B. (2016). US Physician Practices Spend More Than $15.4 Billion Annually To Report Quality Measures. Health Affairs, 35(3), 401–406. https://doi.org/10.1377/hlthaff.2015.1258
Several years ago, I worked with an EHR company to help them develop the logic to drop CPT-II codes automatically.
A clearing house is an intermediate entity between the EHR and the insurance plan. It checks the bills to ensure accuracy and then forwards them to the insurance company for processing.
I successfully resisted the request to submit data in Excel format to the State of CT, since I was faxing the standardized paper form and following the law.
Casalino, L. P., Gans, D., Weber, R., Cea, M., Tuchovsky, A., Bishop, T. F., Miranda, Y., Frankel, B. A., Ziehler, K. B., Wong, M. M., & Evenson, T. B. (2016). US Physician Practices Spend More Than $15.4 Billion Annually To Report Quality Measures. Health Affairs, 35(3), 401–406. https://doi.org/10.1377/hlthaff.2015.1258
Get Started with eCQMs | eCQI Resource Center. (n.d.). Retrieved November 11, 2024, from https://ecqi.healthit.gov/ecqms?qt-tabs_ecqm=about-ecqms
QRDA - Quality Reporting Document Architecture | eCQI Resource Center. (n.d.). Retrieved November 11, 2024, from https://ecqi.healthit.gov/qrda?qt-tabs_qrda=about
Dolin, R. H., Alschuler, L., Beebe, C., Biron, P. V., Boyer, S. L., Essin, D., Kimber, E., Lincoln, T., & Mattison, J. E. (2001). The HL7 Clinical Document Architecture. Journal of the American Medical Informatics Association : JAMIA, 8(6), 552. https://doi.org/10.1136/jamia.2001.0080552
dQMs—Digital Quality Measures | eCQI Resource Center. (n.d.). Retrieved November 11, 2024, from https://ecqi.healthit.gov/dqm?qt-tabs_dqm=dqm-strategic-roadmap
Most current solutions are payer-driven, forcing providers to adapt. The fix isn’t just automation—it’s shifting ownership of the process so that technology works for PCPs, not against them.
If an AI-driven platform could handle retrieval, verification, aggregation, and reporting without constant physician input, it would free up cognitive bandwidth for actual patient care.
The challenge is integration—many of these emerging solutions (eCQM, dQM) still assume physicians will clean up the data mess, rather than designing systems that solve the problem upstream.